Topic: “Patient Advocacy”, QI perspective
Just a reminder, MEQAPI stands for Monitoring & Evaluation, Quality Assurance, and Process Improvement, and you can visit us at http://www.meqapi.org.
In a perfect healthcare world, patient advocacy would perhaps be unnecessary – the processes would place patients at the center, patient goals would automatically be prioritized, and no patient would be subject to care that was not Safe, Timely, Efficient, Effective, Equitable, Patient Centered, and Affordable. No patient would wait unnecessarily, and every illness would attract the right level of funding.
However, that is not the world in which patients actually find themselves.
The world in which they navigate has information gaps and gradients, power dynamics, misleading information, and a hugely complex process that typically prioritizes many other stakeholder’s interests above those of the patient. What the patient encounters is nightmare. Some illnesses take the lion’s share of funding, research, and care, while others languish for want of attention. Very often attention is rationed according to the estimated profitability of treatment, degree to which the condition is emotionally appealing, or just random luck.
Strong patient advocacy can help rectify, mitigate, or avoid the many obstacles, detours, and traps that can prevent a patient from getting necessary care and support.
This week we are discussing patient advocacy with Andrea J. Wilson of Blue Faery. the Adrienne Wilson Liver Cancer Association. Andrea tweets using as @BlueFaeryLiver.
The Adrienne Wilson Liver Cancer Association is writing a Blue Faery Patient Advocacy eBook for cancer patients by cancer patients. The goal of the eBook is to answer commonly asked questions by cancer patients. A writer and editor, President Andrea Wilson is writing the book using personal stories to illustrate specific points. By conducting polls, collecting feedback, and interviewing cancer patients, Andrea is gathering content for the eBook that will be free on Blue Faery’s new website.
Physician’s Weekly have kindly shared the following pertinent articles:
The topic of patient advocacy includes patient/physician partnership, and some medical journals have encouraged research that is done in partnership with patients. The British Medical Journal, for example, maintains a “Partnering with Patients” page.:
The BMJ launched an innovative strategy to promote patient partnership in 2014. It took this step because it sees partnering with patients, their families, carers and support communities, and the public as an ethical imperative, which is essential to improving the quality, safety, value, and sustainability of health systems.
The strategy has seen the journal move to co-produce its content with patients and advancing international debate on how to embed meaningful partnership with patients in clinical practice, service delivery, research, education, and policy. The strategy was drawn up with and continues to be informed by a dedicated international patient advisory panel.f\
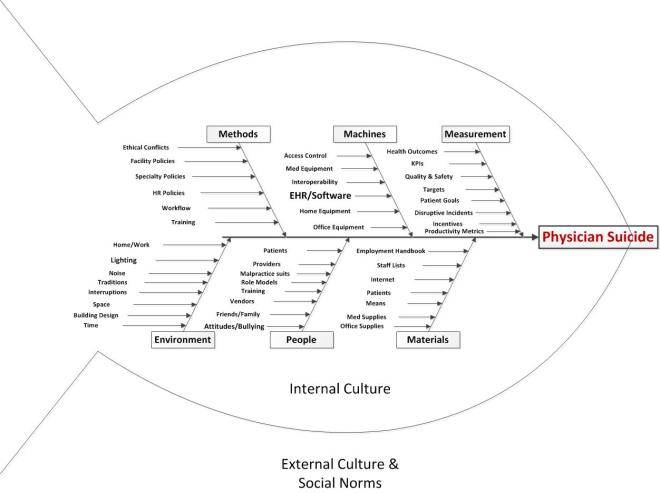
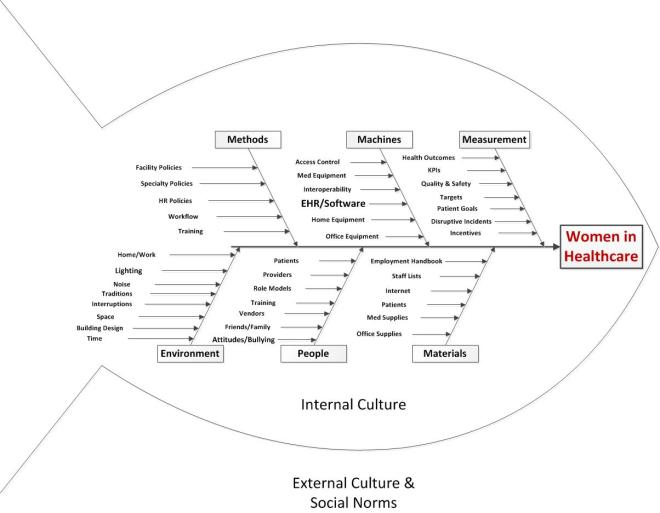
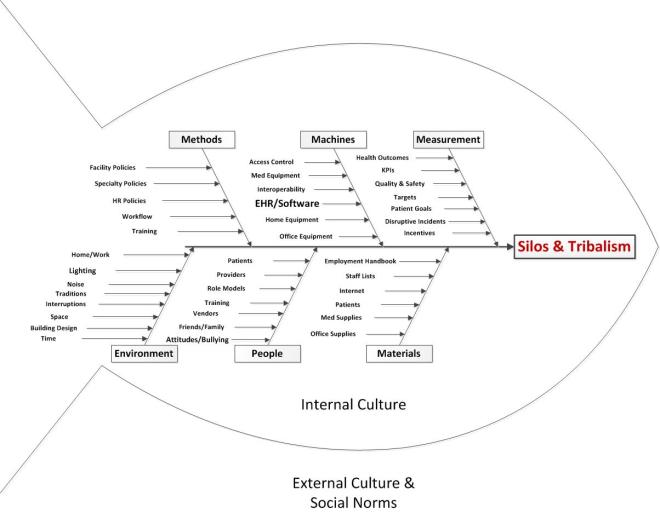
We will take a QI approach, and discuss the topic using each of the typical arms of the basic Quality Improvement Ishikawa diagram to guide and support discussion. An Ishikawa diagram will be provided ahead of time and during the chat.
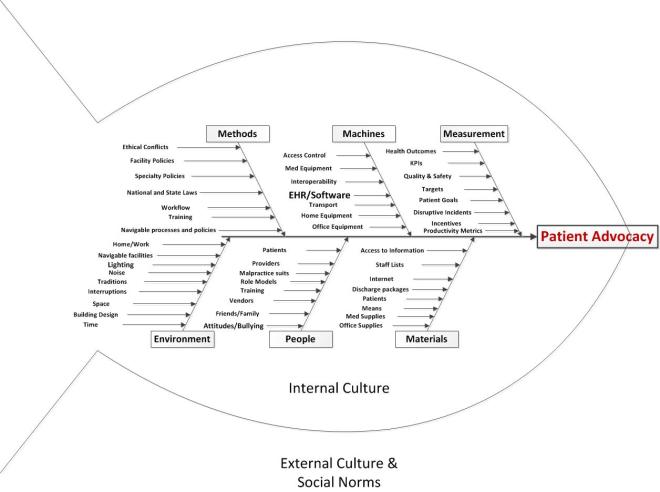
Participants will bring their own experiences, perspectives, and expectations to the discussion, but the topics might break down something along these lines:
-
- Methods
- Policies: office, organization, or national policies, including MU, HIPAA, etc
- Workflow: how things are done including new patient onboarding, care provision, care coordination, ordering/prescribing, billing, patient transfer, etc.
- Workload: demands of the job, and whether they exceed the resources and ability to meet the demand.
- Human Resources Policies, and variation in expectations regarding women and men in the work setting and career progression
- Traditions and memes
- Incompatible policies
- Ability to navigate laws, policies, and processes
- Machines (e.g. equipment, EHR)
- Medical or office equipment
- Home equipment specific to the patient condition
- Integration/interoperation with other office or medical systems, or user personal health records
- Access Control
- Interoperability
- People
- Staffing: sufficient and qualified staff
- Training: base training, ongoing training, CME, and patient or carer training
- Attitudes: staff attitudes
- Fatigue and stress
- Values and traditions
- Friends and family
- Role Models
- Management styles
- Malpractice litigation
- Materials
- Patients: as the “raw material” of the medical process. Patients may come with a range of attitudes, health problems, life situations, and ability to comply with treatment that are challenging and stressful.
- Supplies: medical or office, or self-provided materials, uniforms, personal safety equipment.
- Data: ability to securely share with correct patient, specialist, lab, etc
- Internet sources
- Employment Handbook
- Discharge info packets
- Explanation of Benefits sheets
- Measurement
- Health outcomes
- KPIs: operational metrics required by practice, local government, state, federal
- Quality and safety metrics
- Targets: set by practice, insurer, etc. as well as patient goals
- Incentives and rewards
- Adverse Effects reporting
- Disruptive Incidents reporting
- Productivity metrics
- Patient goals
- Environment
- Noise: distracting noises, sound levels too high, etc. due to computer systems
- Space: Cramped, uncomfortable work space etc. Gender segregated space
- Time: Too little time per patient or order, too little time in a day, too many demands
- Location: things where they should be on the screen, click distance, and location of workstation relative to point of care and patient
- Control: the degree to which the individual can control their workload and how to accomplish it
- Fairness: the perception that the burdens and rewards, the effort and outcomes are spread amongst stakeholders in an equitable way
- Architecture: location of work areas, gathering places, shared areas
- Ability to navigate the healthcare facility
- Methods
Some of the authors of the works cited above may be responding to the following topics, and participants are invited to describe their experiences, and offer their insights and observations.
Topics
- What METHODS influence Patient Advocacy
- What MACHINE factors influence Patient Advocacy
- What PEOPLE issues and expectations influence Patient Advocacy
- What MATERIALS influence Patient Advocacy
- What MEASUREMENT factors influence Patient Advocacy
- What ENVIRONMENTAL factors influence Patient Advocacy
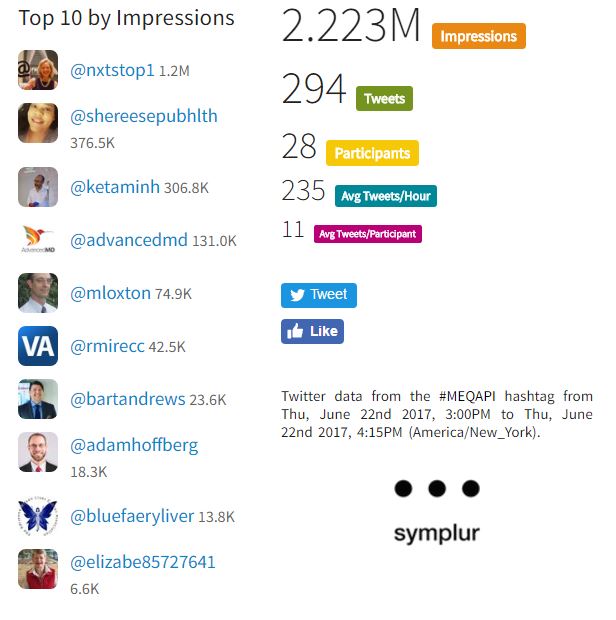
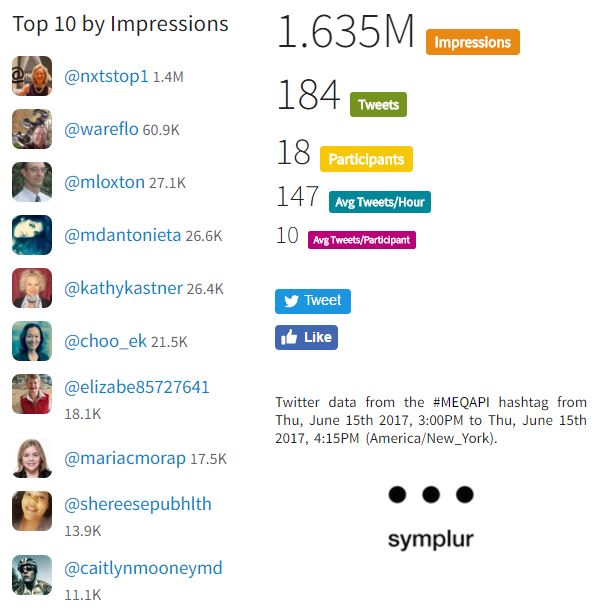
Numbers for last week
Background
MEQAPI focuses on healthcare improvement, and in the spirit of shameless borrowing (and efficiency), takes existing perspectives from the IHI, AHRQ, and others.
To quote the IHI on what the Triple Aim encompasses:
The IHI Triple Aim is a framework developed by the Institute for Healthcare Improvement that describes an approach to optimizing health system performance. It is IHI’s belief that new designs must be developed to simultaneously pursue three dimensions, which we call the “Triple Aim”:
- Improving the patient experience of care (including quality and satisfaction);
- Improving the health of populations; and
- Reducing the per capita cost of health care.
The six domains of care quality (STEEEP) mapped out by the Agency for Healthcare Research and Quality (AHRQ) are foundational to healthcare improvement. All care, and by inference quality measures, should be focused on being Safe, Timely, Effective, Efficient, Equitable, and Patient Centered.
The MEQAPI tweetchat aims to give voice to a broad range of stakeholders in healthcare improvement, and it embraces everyone from administrators to zoologists, and includes physicians, nurses, researchers, bed czars, cleaners, and yes, patients and care-givers.